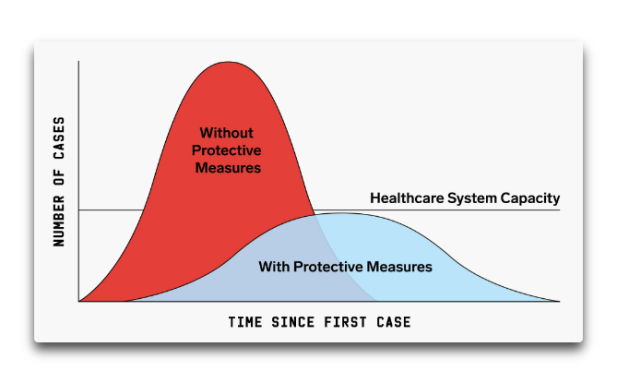
Man, this stuff angrifies my blood mightily. We were sold the idea of “shelter-in-place” in order to “flatten the curve”. This would avoid overloading the medical system, as shown below. Fair enough.
And like a fool, I assumed that when the curve was flattened, we could get back to work.
But noooo … I just got the latest Order of the Sonoma County Health Officer. The shelter-in-place is extended until the following conditions are met to the satisfaction of some County bureaucrat somewhere. The conditions are that before we are free to continue with our lives, Sonoma County must have the following abilities.
• The ability to monitor and protect our communities through aggressive testing, contact tracing, isolating, and supporting those who are positive or exposed;
• The ability to prevent infection in people who are at risk for more severe COVID-19;
• The ability to reduce infection spread so that it is decreasing in the community;
• The ability of the hospital and health systems to have sufficient bed and ICU capacity to handle surges;
• The ability to develop therapeutics to meet the demand;
• The ability to obtain sufficient personal protective equipment (PPE) for hospitals and health system to handle surges;
• The ability for businesses, schools, and child care facilities to support physical distancing; and
• The ability to determine when to reinstitute certain measures, such as the stay-at-home orders, if necessary.
Say what? The pluted bloatocrats of the Sonoma County Government will have to possess all those abilities before they will deign to return our freedom? Some of those are not even possible!
Plus in the last clause, they say they won’t let us go until they can figure out just how and when they can re-imprison us. The mind boggles.
Not only that, but our Sonoma County officials have trouble patching the potholes … no way they’ll EVER have all of the “abilities” listed above.
I’m sorry, but this is simply not legal. These are mere county officials—who made them kings and queens to decide our fate and rule every aspect of our lives?
Oh, yeah, I forgot to mention the so-called emergency. These pinche tiranos claim that their power comes from the corona “emergency”. Sonoma County is home to just under half a million people (494,000). We have had exactly two deaths from coronavirus.
Two.
What kind of a low-budget emergency is that?
Grrrr … seems like its time we stopped listening to these tiranitos repinchitos and just declared the US open for business. Look, we can slow the virus without killing the economy. Protect the most vulnerable, quarantine the sick rather than the healthy, wash your hands (particularly after handling pangolins), wear masks, in social situations stay six feet (2 m) away from bats, and let’s move forward no matter what our self-proclaimed overlords have to say about the matter.
My best to everyone, end the American Lockdown in whole and in part, and most particularly … stay well.
w.




@-WE
“After all, we tried that in New York, which was much harder hit than Alabama, and the hospital got no use at all. None. ”
Do you think it is better to put in facilities that you are fortunate enough NOT to need, or fail to provide facilities that you do end up needing ?
Never let ugly facts get in the way of a ‘beautiful’ theory I guess…
https://www.samaritanspurse.org/article/field-hospital-opens-in-new-york-citys-central-park/
“The Samaritan’s Purse Emergency Field Hospital in Central Park opened on April 1 to care for those suffering with COVID-19. We have admitted 142 patients since we opened and, in general, are treating around 50 patients at any given time.”
LikeLike
izen May 26, 2020 at 6:33 am
Neither. That’s the fallacy of the excluded middle.
I think it’s better to put in facilities that are needed, and not put in facilities that are not needed. As near as I can tell, despite what Mosh said, Alabama is NOT short of ICU beds. In addition, and more importantly, the number of deaths is dropping.
So no, a field hospital is not needed.
w.
LikeLike
“I think it’s better to put in facilities that are needed, and not put in facilities that are not needed. As near as I can tell, despite what Mosh said, Alabama is NOT short of ICU beds. In addition, and more importantly, the number of deaths is dropping.”
MONTGOMERY
MONTGOMERY
not the STATE
the STATE needs ZERO beds
the CITY?
the FUCKING CITY Willis
as for excess capacity? Beijing was great. exces fever clinics were opened. No lines for testing
excess hospitals built for SARS… Opened to accept covid only patients
So my argument.
Montgomery ran out of beds
not the state.
Montegomery.
LikeLike
Steven, the article said that yes, the city of Montgomery was out of ICU beds, but they just moved the patients to a nearby city where there are ICU beds.
So I fail to see what all of your hyperventilating and screaming THE CITY, BOSS, THE CITY are all about. You seem to be obsessed with me and what I say, to the point where you’re losing the plot.
w.
LikeLike
@-WE “So no, a field hospital is not needed.”
I admire your certainty that provision can always exactly match need. But it is misplaced, in reality the ‘middle’ is always excluded when you make provision of inherently uncertain processes.
https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-020-5023-z/tables/3
Hospitals always have more facilities than they need, or a shortage. The chances of them having EXACTLY the number of beds, nurses doctor etc they need is vanishingly small. In most cases they err towards over-provision because it leads to a preferable outcome. Unless you regard the extra expense as worse than a rationed or inadequate response.
It is difficult to make predictions, especially about the future. K.K.S.
LikeLike
Ask willis how well he did
1. predicting case count in Korea
2. predicting deaths in Korea
you do not want him in charge of your public health planning.
Stockpiles?
Here is the Willis logic. I see no cases, why do we need a stockpile?
it is that kind of thinking, that doesnt buy fire insurance, that doesnt get yearly check ups
that doesnt have masks in storage.
By the way, here is a better model
https://www.frontiersin.org/articles/10.3389/fphy.2020.00217/full
LikeLike
Steven Mosher May 29, 2020 at 2:25 pm
OK, let’s look at that once again, seems you’ve forgotten all the times you brought this up before. Back on March 13th, early in the game, I said the following:
Instead, there have been 260 or so deaths. So I’d say I did pretty well, particularly since you predicted that there would be 2,000 deaths, not that I care about such early projections of an unknown virus …
As to the number of South Korean cases, I failed to account for the fact that when testing went through the roof in South Korea, so would the number of cases. I didn’t realize then that looking at cases is meaningless.
Now, this is maybe the tenth time or so that you’ve brought this same meaningless issue up, on my blog, on WUWT, and on Twitter. And each time you’ve done so, I’ve gone through what I actually said. It’s getting boring, and you are starting to look like a vindictive prick who doesn’t care at all about thousands of deaths, you’d rather stand on your tiptoes to try to bite my ankles.
My advice, which you’re free to ignore, is to STOP THE MEANINGLESS ATTACKS ON ME AND GET BACK TO THE SCIENCE.
Just saying, amigo, this sick stalking of me, and your unhealthy obsession with a highly uncertain prediction that I made months ago, a prediction that at the time I said was unlikely to be accurate, is not a good look on you.
The first time you tried this shit it was just ugly.
But after the tenth repetition, it’s sick, sick, sick …
w.
LikeLike
I think Mosher’s problem is that he has excess time to ruminate because he has been in quarantine -t does funny things to your head. And, in accepting his quarantine as ‘normal’ and ‘justified’, he has to justify himself ad nauseum.
The social effects of the ‘lockdown’ in a small town in BC are horrendous with people not just keeping the desired 2m, but avoiding eye contact. It seems as though the government spun fear has broken normal social conventions. The brown paper in store windows is telling of business failures. As we ‘reopen’ stories of people who refuse to return to work are accumulating, as a consequence of Trudeau’s $2K/m which has just been extended into July. Now I am getting scared, and its not the Wu Flu that worries me.
LikeLike
See, Willis – your ducking has nothing to do with me.
> After all, we tried that in New York, which was much harder hit than Alabama, and the hospital got no use at all. None. ”
> > “The Samaritan’s Purse Emergency Field Hospital in Central Park opened on April 1 to care for those suffering with COVID-19. We have admitted 142 patients since we opened and, in general, are treating around 50 patients at any given time.”
Nothing to do with me.
LikeLike
Nope. I was referring to this $21 million coronavirus hospital just built in New York, that just closed without ever seeing a patient …
w.
LikeLike
yep.
a great example of what can work
Now, they should have used it for THE ELDERLY AND NOT SENT THEM BACK TO CARE FACILITIES.
I am going to have my house burned down because I paid for fire insurance and never used it.
So build a field hospital for MONTEGOMERY.
can you fill it?
yep. If not with ICU patients, then you can isloate some of the positive there.
Today, people who test positive are sent home to infect their family.
DUMB
LikeLike
Steven Mosher May 29, 2020 at 2:30 pm Edit
Should we build field hospitals for every city in the US?
Obviously not. And most particularly, building them now after the peak has passed almost everywhere is likely a waste in most cases. So we need to put them in the places where there is actual need.
Meanwhile, Alabama has a covid death rate of 123 per million. The US average death rate is 392 per million, more than three times that of Alabama. And there are no less than eight states with death rates over 500 per million.
So perhaps Montgomery is not where we might want to put our time and treasure … let them move covid patients to nearby cities. We’ve already wasted enough money on this madness, at some point we need to back up and think about where we can get the most bang for the buck.
Which might be Montgomery … or not …
Regards,
w.
LikeLike
“Should we build field hospitals for every city in the US?
Obviously not. And most particularly, building them now after the peak has passed almost everywhere is likely a waste in most cases. So we need to put them in the places where there is actual need.”
#############
1. if you wait for the need to develop it is too late.
2. So you have to make bets.
3. You probably want to make bets on places that came close to over topping their capacity.
4. the CDC has a metric you want to hit: 30% spare capacity
5. you probably also want to make bets in places that
A) ran close to over topping
B) are opening while their RT is going up Alabama is Rt of ~1.04
Look. this is not hard. when we build dams we dont wait to see how they get flooded. SOMEONE
has to plan. someone has to decide based on limited amounts of bad data how high to build the dam
or How many hospital beds to have.
THAT PERSON WILL ALWAYS BE WRONG. they will always build too little or too much.
Its not that hard to put up an emergency hospital
“https://www.israel21c.org/how-to-build-an-emergency-field-hospital-in-12-hours/”
and Hope you dont need it
LikeLike
Deconstructing ideologically- driven simplistic narratives is always a good thing:
–snip–
The question is: is any of this true? Did the modelling, as the Daily Mail put it last Saturday, “single-handedly (trigger) a dramatic change in the government’s handling of the outbreak”? If the code is so bad, does that render the modelling useless? And would shoddy modelling remove the justification for the lockdowns in place across much of the globe anyway?
https://ftalphaville.ft.com/2020/05/21/1590091709000/It-s-all-very-well–following-the-science—but-is-the-science-any-good–/
LikeLike
My comment is indirect regarding your posts on “watts up with that, Daily #Coronavirus #COVID-19 Data Graph Page“ I look forward to your updates. I like your analysis skills and related analysis.
I have a suggestion. Is there a way to run an analysis based with latitude as a variable? I have noticed most of the large population states that are higher than 40 degrees north like New York and Michigan have very similar high rate peaks whereas lower latitude states have Lower broader rate peaks. There would need to be some criteria to only include sufficient population or data.
Obviously, I am thinking of the vitamin D from sunlight factor. Thanks
LikeLike
Thanks, mddwave. The issue with comparing countries by latitude is … on what basis are you going to compare them? I suppose total deaths per million might do it. And then, of course, in addition to latitude we have half the world in summer (extra vitamin D) and half the world in winter (not enough Vit. D).
Next, although over the year the total amount of daily sunlight is related to the latitude, on any given day it’s a function of latitude and solar declination.
Finally we have the issue of the relative wealth of the country … wealthier countries won’t have as high a death rate, and the wealthiest countries are generally in the northern extratropics, which will screw royally with any analysis …
Not sure how I’d untangle that box of snakes to give any significant answer.
w.
LikeLike
I don’t think it’s worth trying to track weather related issues. but if you were to do this based on sun angle (latitude adjusted for tilt), that would handle the north/south hemisphere issue, with say april 1 as a fair midpoint.
one other problem with considering V-D is that thelockdown orders keep people inside away from it.
LikeLike
Willis, there are many interesting trends and facts to be stressed in recent Covid figures.
– UK is now above Spain for fatalities per population , so did not take any advantage of the experience of countries like France, Italy, Spain where pandemic started/accelerated earlier; it may be linked to the lack of early Covid treatment through HCL/AZT
– Sweden is now above France, with still a worrying trend; the local guru is realizing his country perhaps did not make an optimal strategy choice;
– the US remains far below Sweden, but are now closer to Ireland; there are still many states with 5% positive cases among tested people; very high compared to NY, or Marseille area in France where the ratio is @ 0,5%´
LikeLike
Willis, there are many interesting trends and facts to be stressed in recent Covid figures.
– UK is now above Spain for fatalities per population , so did not take any advantage of the experience of countries like France, Italy, Spain where pandemic started/accelerated earlier; it may be linked to the lack of early Covid treatment through HCL/AZT
– Sweden is now above France, with still a worrying trend; the local guru is realizing his country perhaps did not make an optimal strategy choice;
– the US remains far below Sweden, but are above Ireland and the Netherlands; there are still many states with 5% positive cases among tested people; very high compared to NY, or Marseille area in France where the ratio is @ 0,5%´; see:
https://www.mediterranee-infection.com/covid-19/
Do you monitor also the number of testing per state? It may be that testing policy is changing, leading to positive ratio having limited meaning.
We saw that in France where -apart from Marseille area- clinically ill persons were at some point no longer tested. Now testing became the national norm, and the positive ratio is around 1%
Best. Daniel
LikeLike